

Evaluating the Science of Covid Vaccine Mandates
Evaluating the Science of Covid Vaccine Mandates
What do the data say about the efficacy and safety of Covid Vaccines?

It seems that every single mainstream source and most governments and institutions around the world are coercing people into getting the Covid-19 vaccine. They claim that it is a question of public safety. While it is true that no individual can be coerced into a medical intervention against their will, these institutions claim that it is important to put human rights and freedoms to the side in this instance because one person choosing to refuse the intervention ostensibly affects the health of others. Those who refuse or protest this coercion are labelled “Anti-science” and dangerous individuals. So, let us explore the scientific evidence behind this premise and evaluate whether or not it is true that it is necessary to get the vaccine.
There are a few reasons, we are told, that it is necessary to get the Covid-19 vaccine:
It can prevent you from getting Covid-19.
Even if you yourself don’t care about getting sick, it can prevent you from spreading Covid-19 to others who may not be able to survive the symptoms.
A majority of the population must become vaccinated in order for the vaccine to work.
In this Substack, I will explore the science behind all of these claims and evaluate whether these reasons are true, or whether they are anti-science by people who know how to lick boots but never actually learned any science on their way to PhDs, MDs and blue checkmarks.
Reason number 4, by the way, that most people are getting vaccinated, is so that they can get back their basic freedoms. This is the saddest reason of all. It means you are being medically raped and letting it happen because you convinced yourself that you have no power.
Section 1: Vaccines are not effective in preventing infection, or in protecting people from the symptoms of covid-19.
The theoretical function of vaccination is as follows: a diminished and therefore non-functional version of an offending virus is injected into an individual with a functioning immune system. The immune system then recognises this non-functional version of the virus as "non-self" invader and raises an attack against it. B-cells are created that will "remember" the virus through biological mechanisms which will permit the body to more quickly recognise the real virus if they are ever infected in the future and therefore be able to manage the infection more efficiently. Therefore, a vaccine cannot prevent infection, even theoretically; it can only ever diminish the symptoms. Nevertheless, an unscientific narrative about vaccines has been permitted to be promulgated by public health authorities that misinforms the public that vaccines can prevent infection. Entire health policies are made based on this misinformation.
Fortunately, we can test the unscientific claim that a vaccine prevents the transmission of disease from one person to another in a community where most people are vaccinated. The most vaccinated countries in the world are: Gibraltar, Malta, Iceland, UK, Israel, and Seychelles. Gibraltar has a 100% vaccination rate (Fig 1). Regardless, the country is experiencing an alarming rise in Covid-19 cases of which 74% of these cases are in fully vaccinated individuals (the unvaccinated are not citizens, but rather visitors to the country) (Fig 2). Malta is the second most vaccinated country in the world with 90% of the population vaccinated by July 28, 2021 (Fig 3). On July 7th however, Malta began experiencing massive spikes in Covid-19 cases (Fig 4). In Iceland, 75% of the population is fully vaccinated and 70% had at least one dose (Fig 5). in June 2021, cases were rising among both the vaccinated and unvaccinated population (Fig 6).

Fig 1. Share of the population (of citizens) in Gibraltar that is fully vaccinated is at 100%. The only unvaccinated people are tourists that make up a very small percentage of the total population.
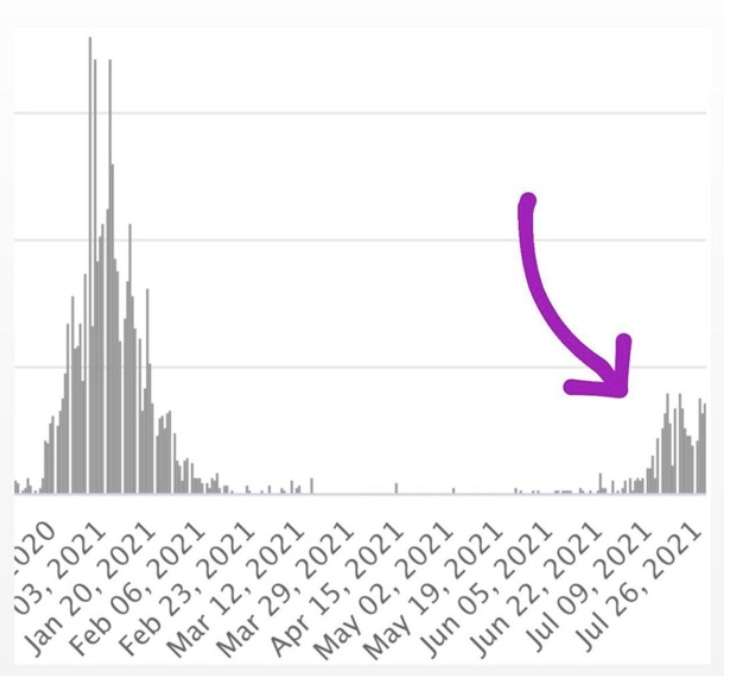
Fig 2. Despite this mass vaccination success in Gibraltar, it is currently facing a massive Covid-19 surge in incidence.
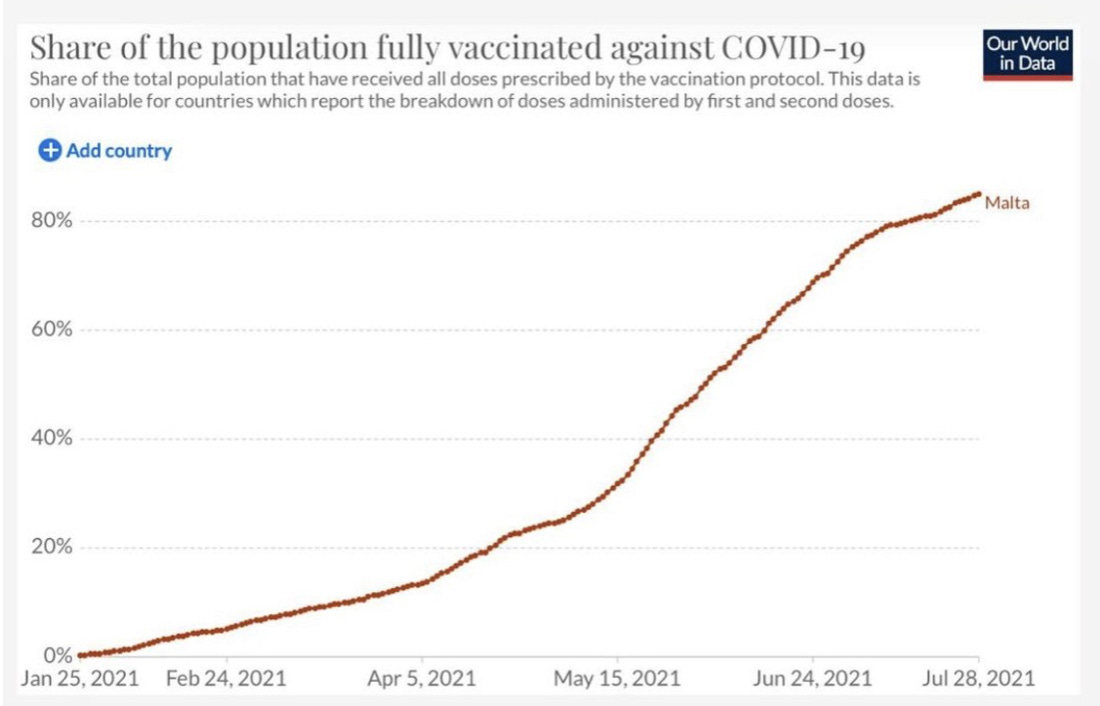
Fig 3. Malta also had a very successful Covid-19 vaccination campaign and got 80% of its population vaccinated.

Fig 4. Nevertheless, Malta is currently facing a massive surge in Covid-19 cases.

Fig 5. The fully vaccinated make up a large proportion of the number of covid cases in Iceland. Suggesting that being fully vaccinated does not protect a person from becoming infected.

Fig 6. The UK has 60-70% of its population vaccinated.

Fig 7. Yet the number of new cases among the vaccinated and the unvaccinated is identical and in fact seems to be increasing among the vaccinated.

Fig 8. Public Health England reports that the fully vaccinated actually have the same viral loads as the unvaccinated.

Fig 9. Vaccination rates were the same inside and outside the GTA (greater Toronto Area) in Ontario, Canada. Yet, the death rates due to Covid-19 were greater in the GTA compared to outside. This means that vaccination rates do not affect mortality from Covid-19.

Fig 10. Pfizer’s six month safety data trial reveals that the vaccinated and the unvaccinated are equally as likely to die from Covid-19. This means that getting the vaccine to mitigate symptoms or mortality from the disease is not supported by evidence and is therefore untrue.
What can we learn from this data?
Based on the fact that countries with 100% or near 100% vaccination status experience huge spikes in covid cases, especially among the fully vaccinated, we can conclude that the idea “if everyone gets vaccinated, we can stop the spread of this disease” is incorrect. (Fig 1-4)
Based on the fact that the fully vaccinated are getting Covid-19 at the same or higher rates than people who are unvaccinated, we can conclude that being fully vaccinated does not protect a person from getting Covid-19. (Fig 5-7)
Based on the fact that vaccinated and unvaccinated individuals have the same viral load, it means that vaccinated and unvaccinated individuals hypothetically have the same capability to spread the disease. This means that excluding people for being unvaccinated because they might infect people is ludicrous as they have the same ability to infect others as fully vaccinated people. (Fig 8)
Based on the fact that mortality rates from Covid-19 are the same among vaccinated and unvaccinated populations, it is not scientifically supported that vaccination mitigates symptom severity or mortality from Covid-19 (Fig 9).
Section 2. Vaccines can cause serious adverse events to people. These side effects are not made known to the common person, violating their right to informed consent to medical interventions.
The purpose of getting the vaccine was to mitigate symptoms, spread and deaths from the disease Covid-19. However, as the data have demonstrated in Section 1, the vaccine does not achieve any of these end points. The side effects of the vaccine therefore, although previously could have been balanced against its benefits, now are shown to be even more egregious. There is no good reason for any person to tolerate these side effects. There is considerable evidence that Covid-19 vaccines are not merely useless, but also harmful to people.
Vaccine effects on Fertility
The vaccine consists of a lipid nanoparticle (LNP) which contains this mRNA strand encoding spike protein. The LNP permits this mRNA to enter into cells of the patient's body where it will be used to manufacture the spike protein. The idea of this form of "vaccination" is that the body will produce its own spike proteins and then launch an immune attack against anything that expresses these proteins. This is thought to train the immune system to combat a future infection of coronavirus which will also express spike protein. The spike protein, wherever it is produced, launches a violent inflammatory reaction. The LNP enters cells in the body using ACE2 receptors which are over expressed in some key areas of the body such as the reproductive organs (ovaries, testicles), liver, and lungs.
Damage to fertility is a primary reason for vaccine hesitancy among those in their reproductive age. Mainstream media and science present the narrative that these concerns are unfounded and unscientific. However, there is evidence for the dangers of lipid nanoparticles for fertility. In a Confidential Pfizer Research document, it is revealed through radio-label testing that the vaccine tends to accumulate most in the liver, spleen, adrenal glands and ovaries most of all. The lipid nanoparticle coat permits the vector to enter more cells.
https://rightsfreedoms.wordpress.com/2021/06/03/confidential-pfizer-research-document/
The spike protein is known to be pro-inflammatory and will therefore cause inflammatory reactions to occur in the ovaries that can damage or destroy inchoate follicles.
Shahanshah Khan, Mahnoush S Shafei, Christopher Longoria, "Spike protein induces inflammation via TLR2 dependent activation of NFkB pathway".
The spike protein shares a domain sequence with the protein syncitin-1 which is involved in early fetal development. Researchers have tested and concluded that in vaccinated pregnant and non-pregnant women, the women did not develop anti-syncitin 1 antibodies. However, this study does not complete any functional assay and therefore its conclusion about the safety of the vaccine are premature if not unfounded. A functional assay would determine whether or not the syncitin protein function is still being carried out properly in unvaccinated women. Just because her body is not producing antibodies against syncitin 1 doesn't mean that the vaccine is not deleterious to trophoblast/placenta.
A functional assay must be done that incubates trophoblast/placenta tissue with the vaccine and observes the interaction between the two to determine for certain that there is no impact that the vaccine has on the placenta health. Without this assay it is not only irresponsible, but also scientifically negligent to make such a bold statement as saying that the vaccine has "no effect on fertility" and that the hesitancy among reproductive aged and pregnant women is unfounded.
CNZ Mattar, Winston Koh et al. "Addressing anti-syncitin antibody levels and fertility and breastfeeding concerns following BNT162B2 Covid-19 vaccination" medRxiv https://www.medrxiv.org/content/10.1101/2021.05.23.21257686v1.full-text
Scientific evidence supports the fact that vaccination poses a significantly elevated risk of miscarriage in pregnant women. Data on pregnancy loss are based on 827 participants in the v-safe pregnancy registry who received an mRNA Covid-19 vaccine (BNT162b2 [ Pfizer--BioNTech] or mRNA-1273 [Moderna]) from Dec 14 2020 to Feb 28 2020 and who reported a completed pregnancy. A total of 700 participants (84.6%) received their first eligible dose in the third trimester. Data on neonatal outcomes are based on 724 live born infants including 12 sets of multiples.
A total of 96 of 104 spontaneous abortions occurred before week 13 of gestation. The denominator includes only participants vaccinated before 37 weeks. They report 12% miscarriage rate by comparing the number of miscarriages in the first trimester to the total number of pregnant women who were vaccinated: 104/827. However, all the miscarriages occurred in the first trimester and only 127 women were vaccinated in that time period. Therefore, including women who weren't even vaccinated in the first trimester is disingenuous because they technically are not in the group of "vaccinated pregnant women" at that point. The correct comparison would be 104/127=81.9% of women who got vaccinated in the first/second trimester experienced a spontaneous abortion.
This is an alarmingly high rate of miscarriages. To pretend that this is not linked to the vaccine is ridiculously disingenuous considering how much higher this statistic is compared to the normal rate of miscarriages. In fact, it would require formidable evidence to refute that these miscarriages were caused by the vaccine. If something is bad for a baby in utero, it is usually safe to assume that it is also bad for us as human beings. It is simply that we, as developed adults, tend to be more resilient against toxins than babies are.
It is impossible to tell the long term effects of this medical intervention because it has not been tested over a long enough period of time. As such, it is impossible to tell what the effects of the vaccine will be on the reproductive organs over time. It is possible that the inflammatory response in the ovaries and testicles of vaccinated individuals may not be symptomatic until later on. It is prudent to be cautious about such effects because fertility is something that, once lost, is difficult to regain and can change the course of someone’s life forever.
There are many medications that impact our fertility. One example is chemotherapy medicine. This medicine is given to extremely sick patients who require the benefits of the medication in order to recover from cancer. I will not debate the efficacy of this treatment here but use it merely as an example. This treatment does show some degree of success in shrinking and eliminating tumours from suffering patients, even if it damages their reproductive organs in the process. So why do the patients go through with it? Because they are sick.
Perfectly healthy people are being coerced to take the covid-19 vaccination, at the risk for their fertility and health, in order to give others the illusion of feeling protected. The scientific data demonstrates clearly that this trade off is not even worth it, because the vaccination protects no one.
Functional Neurological Disorders
There are also many other side effects to the vaccine that have been reported. One of these are Functional Neurological Disorders. A functional neurological disorder is a disruption in normal brain mechanisms for controlling the body. It includes symptoms such as sensory abnormalities, gait or balance disruptions, or weakness. Patients with functional disorders following their second dose of the Covid-19 vaccine have been reported in a correspondence published in Movement Disorders.
"The first patient presented with a short episode of generalized tonic-clonic psychogenic non-epileptic seizures (PNES) 20 min after receiving the second dose of the Pfizer vaccine. The event was followed by different episodes with different phenomenology such as the inability to move the whole body with a preserved level of consciousness."
"The second patient showed persistent dizziness and a subjective loss of tactile sensitivity in the right arm and leg two weeks after receiving the Astrazenica vaccine."
"In our view FND following Covid-19 vaccination will not be a rare phenomenon and will be widely covered by the media, being interpreted as a direct consequence of the vaccine, as already seen in the past."
The authors clearly describe numerous incidences of FND at various time points following vaccination but baselessly assert that these FND symptoms have nothing to do with the vaccination. In order to say that an effect was NOT cause by the vaccine, the researchers would have to prove that there is no causal link for example by revealing a different cause for the FND such that it occurs independent of the vaccine at the same frequencies. The authors suggested that stress could be a cause but offer no scientific evidence for this such as an experiment or study that showed that FND occurs at the same frequencies in unvaccinated individuals who are experiencing stress.
Alfonso Fasano, Antonio Daniele "Functional disorders after Covid-19 vaccine fuel vaccine hesitancy". Correspondence to Professor Alfonso Fasano, Movement Disorders Centre, Toronto Western hospital 399 Bathurst St. 7MCL410 Toronto ON, CA. http://dx.doi.org/10.1136/jnnp-2021-327000
Butler M et al. "Functional neurological disorder after SARS CoV 2 Vaccines: two case reports and discussion of potential health implications" J. Neuropsychiatry Clin Neurosci 2021
A running theme one notices in the discussion of vaccine related side effects is their so-called rarity. Even if a side effect is rare, it is important to determine a way by which we can determine if there are any factors that predispose someone to experiencing these "rare" side effects.
If a side effect is functional neural degeneration for example, then it should be revealed to patients that the true rates at which this occurs. Asserting that it is not caused by the vaccine with no evidence is not only unscientific, it is dangerous and malicious. All medical interventions have some side effects. The patient decides to take on these side effects in order to get the benefits of the medication. However, if it is known that the vaccine offers no benefit either to the individual getting the vaccine or to the community as a whole, then it is ludicrous to ask them to take on the risk for the side effects, however rare or inconsequential they may be.
Section 3. Cost Benefit Analysis: Was the pandemic killing people or were lockdown restrictions?
Not everyone who receives the vaccine experiences the same side effects. Why is that? Because people have different bodies that respond in different ways. If you were to be put into a gymnasium with 900 people, and be told that one person would die from the injection that everyone receives, would you stay in that place and get the shot? Perhaps. Only if not getting it actually meant that you had a higher than 1/900 chance of dying. As it stands, the statistic for deaths from covid are much much lower than 1/900. In fact, they are almost non-existent if you are a healthy person living a health lifestyle. It is therefore unethical, illogical and unscientific to coerce you to get the shot.
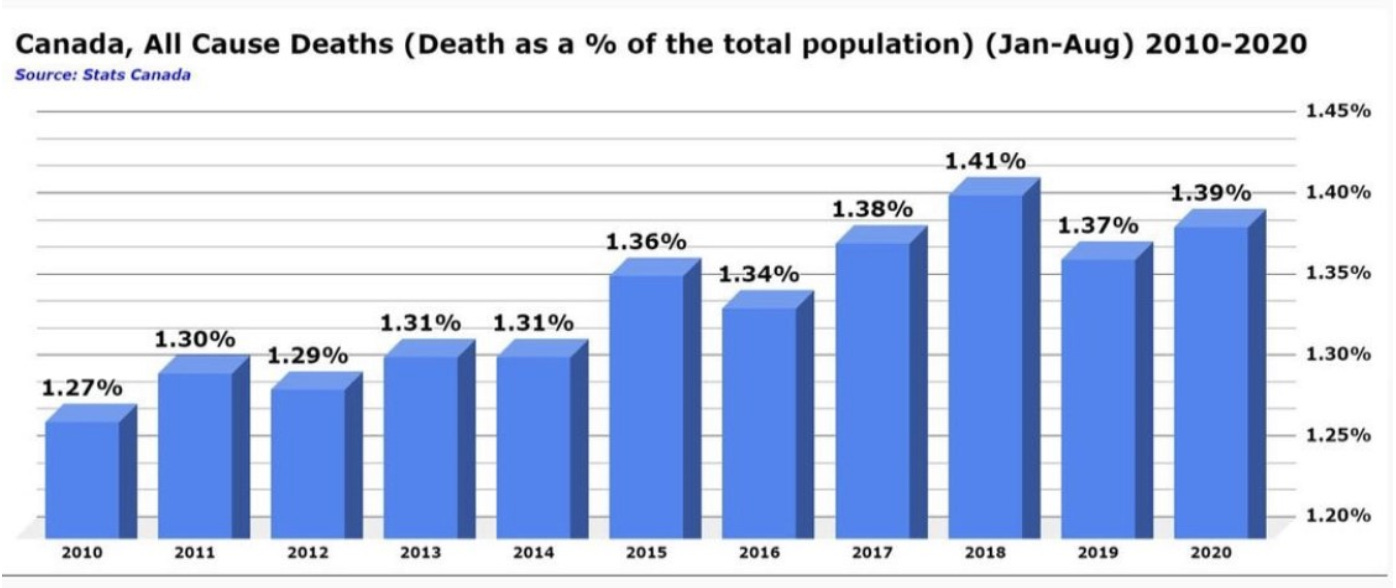
Fig 10. The Covid-19 Pandemic itself may be called into question considering the number of deaths in 2020 compared to other years is largely unremarkable. If there were truly a pandemic, we would be able to see a clear rise in deaths in the year 2020 compared to others. Source: Stats Canada
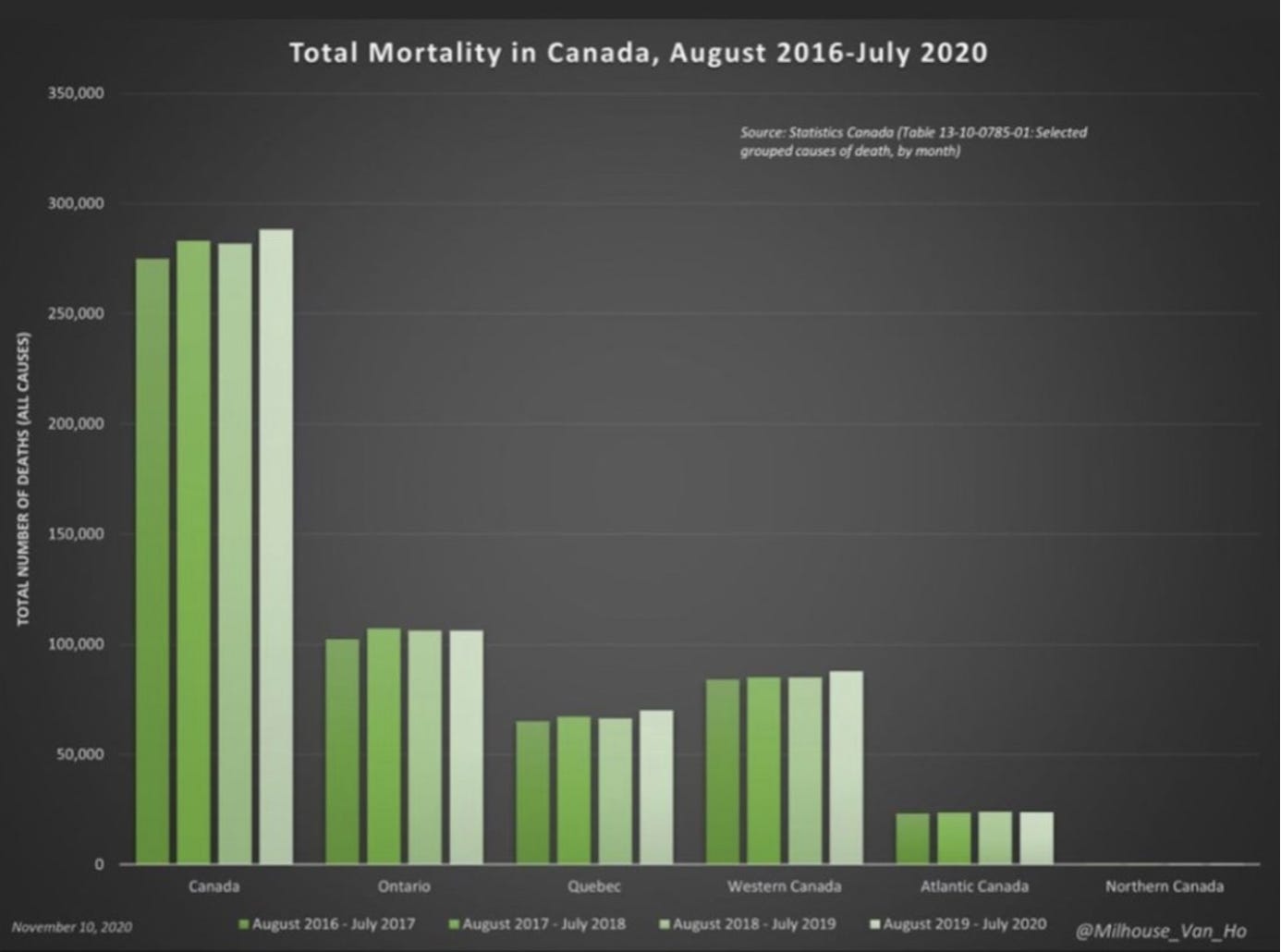
Fig 11. The number of deaths during the months when the pandemic was supposedly rampantly killing people are also unremarkable compared to other months of the year, in all of the provinces of Canada.

Fig 12. Weekly all cause deaths due to Covid-19 are insignificant compared to normal. The pandemic is not as deadly as the media makes it out to be. Source: https://t.co/sDGQltJapg?amp=1 , https://t.co/Qh0WO84rkl?amp=1
If there were truly a pandemic that was killing many people, one would expect that there would be a large number of excess deaths due to Covid-19. This, however, was not the case according to the data.
Excess deaths is an increase in the number of deaths that occur in a given time frame, when compared to the average number of deaths that occurred in the same time frame in the past. Between March 15 and April 25 2020, British Columbia recorded 372 more deaths than in any of the previous five years for these same weeks, but just 99 of those were Covid deaths. This means that the lockdown measures were undoubtedly responsible for these deaths through mechanisms such as delayed treatments for non covid related medical interventions, isolation related drug overdoses and neglect for those who depend on the community, loneliness related suicides and many more. In Alberta, during 7 weeks of isolation, there were 402 additional deaths but only 40 were related to Covid-19. (Source: Our World in Data, Woolf SH et al 2020).
In a report from the Journal of American Medical Association, it is reported that between March 1, 2020 and April 25 2020, a total of 505059 deaths were reported in the US. In 14 states, more than 50% of excess deaths were attributed to underlying causes other than Covid-19. The 5 states with the most Covid-19 deaths experienced large proportional increases in deaths from non-respiratory underlying causes including diabetes (96%), heart disease (89%) and Alzheimer’s disease (64%). The authors suggest that restrictions imposed by governments in response to the pandemic such as stay at home orders could claim lives indirectly through delayed care for acute emergencies, exacerbations of chronic diseases and psychological distress.
Indeed, lockdown and quarantining of asymptomatic Covid-19 patients is unscientific and therefore immoral. Dr. Maria Van Kerkhove, head of WHO’s emerging diseases and zoonosis unit said at a new briefing from the United Nations agency’s Geneva Headquarters, “From the data we have, it seems to be rare than an asymptomatic person actually transmits onward to a secondary individual”.
Source: Woolf SH, Chapman DA, Journal of American Medical Association. July 1 2020. “Excess deaths from Covid-19 and other causes, March-April 2020”.
Fig 13. https://t.co/V9Ao9gIUGo?amp=1
Many of the deaths that the world has been facing in 2020 and 2021 have been due to lockdowns rather than due to Covid-19 itself.
“Hospital Burdens”
Many of the restrictions that were placed on people’s lives during the last two years have been done supposedly to limit the number of people who become sick and have to be admitted to the ICU. However, the ICUs have been at the same capacity as they always were every other year regardless of the degree of lockdown restrictions placed on people. In fact, most of the people admitted into ICUs are not even Covid-19 patients. They are merely tested for Covid-19 after being admitted and it comes back positive.
According to uhn.ca, in three hospitals in Toronto’s University health system, there were 10 patients admitted to the hospital for Covid-19 and under 10 in ICUs while the population of Toronto is over 2 million. If the ICUs are overwhelmed by 10 patients, perhaps the problem is that hospitals must be built to accommodate more patients that would better serve a population of more than 2 million.
Fig 14. The ICU admissions and hospitalisations during Covid-19 have not exceeded nor even reached peak levels that are normally experienced by Ontario during normal flu and pneumonia outbreaks. Yet Covid-19 seems to merit a complete upheaval of people’s lives.
Quarantining healthy people, social distancing and lockdown are policies that are unscientific and unsupported by data. In a meta-analysis of 98 studies, 79 of which were about SARS CoV-2, they investigated evidence of pre-symptomatic spread. People who are perfectly healthy and have no symptoms are mandated to quarantine at the caprice of the government’s decisions. The study reports however that “although modelling studies estimated potential viral load peak before symptom onset, we did not identify any study that confirms pre-symptomatic viral load peak”.
Source: Muge Cevik, Matthew Tate, Ollie Lloyd, et al. The Lancet. Nov 19 2020. “SARS CoV2, SARS CoV, MERS CoV viral load dynamic duration of viral shedding and infectiousness: a systematic review and meta-analysis”.
Section 4. Anecdotes of Harm
Every medical intervention, including vaccines, have some adverse events for a proportion of the population. When a new medical intervention is introduced to the public, it is therefore important to evaluate:
what are the risks associated with the intervention
what percentage of the population is likely to experience these adverse events
how can we identify those people who are most likely to experience these adverse events?
Such an investigation is necessary because it comprises the ability to give informed consent to a patient. It is not only the patient’s prerogative, but his responsibility to determine whether an intervention will harm him, in what way, and whether or not this is worth the benefits of the intervention to him. Without these rights, it is quite easy for unscrupulous mercenaries to take advantage of vulnerable, sick people, by selling them ineffective medications without regard for risk to the patient. Without these standards and the defence of the patient’s rights, modern medicine cannot be trusted as a scientific institution.
VAERS
There is evidence that the Vaccine Related Adverse Event System (VAERS) under-reports the true proportion of the population that suffers from adverse reactions to the covid-19 vaccine. A study to evaluate data collection tools to improve the safety of national vaccination programs reports that “Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious adverse events are reported.”
There was a conflict in the proportion of a certain type of adverse events reported in VAERS, namely anaphylaxis. This discrepancy can be used to determine the true number of people who have died from the Covid-19 vaccines and experienced adverse events. The first JAMA article (The Journal of American Medicine Association) was published in January 2021 and cites 2-5 adverse events/million according to VAERS. The second JAMA study was published in March 2021 and it demonstrated that anaphylaxis occurs in 2.47/10 000, a rate much bigger than the 2-5 adverse events/million. The contradiction implies that VAERS is underreporting by 50-120x.
As of March 2021, VAERS reported 50716 adverse events from covid-19 vaccines which included 1785 deaths. This means that the true number of people who were injured is 5, 071,600 and the true number of deaths due to vaccines is “178500”.
Kimberly G Blumenthal, Lucy R Robinson et al. JAMA (March 2021) 323(15):1562-1565. “Acute allergic reactions to mRNA vaccines.”
Tom T Shimbuko, Matthew Cole. JAMA (November 2021) 325(11): 1101-1102. “Reports of Anaphylaxis after receipt of mRNA Covid-19 vaccines in the US—Dec 14, 2020 - Jan 18, 2021.”
Anecdotes
There is a massive collection of anecdotes shared throughout social media on the internet regarding people’s personal stories about their negative reactions from the vaccine. These stories have largely been silenced or removed from the internet because they “encourage vaccine hesitancy” and authorities suggest “there is no way to link the reaction to the vaccine causally”.
Let us do the logic through these statements to think about whether they are reasonable.
What is data? Data is information. Data from an experiment can give you information about the behaviour of variables in a specific, controlled context. External validity is the ability of the data from the controlled context, to tell us about how the variable will behave in reality, where there are many other variables to interact with. This means that the behaviour of the variable in the real world may or may not be the same as it was in the experiment.
Anecdotes are not “scientific” because the phenomena occur in uncontrolled conditions with arguably an infinite number of variables interacting with each other. For example, a person who takes an aspirin and his headache goes away may not for sure say that his headache went away because of the pill. It could have gone away on its own anyway, it might have been the food he ate differently that day, a difference in mood, drinking the glass of water with the pill, taking a nap after eating the pill. There are a number of factors involved that are not controlled. However, we do not reasonably entertain these alternative hypotheses.
If millions of healthy people take some medical intervention and a short time afterwards, a significant proportion of them begin to develop similar symptoms, we should look into the phenomenon. It is true that sequence alone does not imply causation. However, it is a possibility. Of all the variables in the person’s life that could have caused the symptom they experienced and blamed on the vaccine, the vaccine is one of them. As such, it is a suspect that should be fairly assessed. Compared to the other variables in the person’s life that could have caused the incident, the vaccine is the only variable that is new.
The burden of proof, in fact, is on the vaccine manufacturers to prove that it is SAFE and not on the patient to prove that it is unsafe. Especially when it is being mandated to the public.
BigData Cancels Noise
When a large enough set of data is collected, the noise, because it is random, cancels itself out. If there is any signal (in this case, any relationship between the vaccine and the adverse events reported by anecdote) then it will be amplified. It is quite suspect, then, that people are not invited to share their perceived adverse events more and instead are silenced. The only reason someone would want to silence this kind of information from being documented is if they didn’t want to risk results that might say that the vaccine is, in fact, deleterious to health.
Conclusions
We must make public health decisions based on sound, scientific data.
According to the data, there are a few things that are absolutely clear:
The Covid-19 pandemic was not more lethal than normal flu seasons. Most of the excess deaths during the pandemic were due to lockdowns and their consequences. Hospitals are as full as they have ever been every other non-pandemic year. Most of the patients filling up the ICU are there for non Covid related reasons, but test positive anyway and then are labelled Covid patients, artificially inflating hospitalisation stats.
The Vaccine does not prevent infection or decrease chances of hospitalisation from Covid-19. An unvaccinated person has the same viral load as a vaccinated person and therefore, the same ability to “spread disease”.
The vaccines pose dangers to some significant proportion of the people who take them and as of now, it is impossible to tell who will respond in what way. The lack of knowledge on the safety of this intervention is even more egregious considering it is neither efficacious nor necessary.
Death, long term negative health effects, and health system burden from Covid-19 is almost 0% in people who are healthy and young. The common denominator among people who are hospitalised for Covid-19 symptoms is obesity and vitamin D deficiency.
As such, the known and unknown risks from a vaccine are unwarranted for everyone. People who are at risk for severe covid-19 symptoms have no guarantee of protection from Covid-19 and taking the vaccine only adds for them the risks of the vaccine itself.
The Vaccine Sets a Precedent
The people who take the vaccine, in order to keep a job, travel, continue living their normal life and to just “not have to think about Covid-19 anymore” do not realise that this does not stop with the vaccine.
Once an governing institution has the capability to take away your ability to work, use public transportation, travel, and access your basic rights and freedoms as a human being, for a vaccine, they can do it for any law or mandate they deem necessary.
Anyone with enough money and power to influence the government can mandate their product at pain of death for the entire population. What an excellent business model. If you, whether you are for or against the vaccine in particular, do not stand up to this mandate, then you are signing away your rights in the future as well.
All virtues are tested the they are difficult to wield. Now is the time when courage is challenging, but it is a matter of life and death. Do you wish to die honourably, with a sword in your hand, or like a coward who in inches and doses, sold his spirit for a bit of false security?
There is a reasonable evidence that some vaccines work. Pfizer-BioNTech, Moderna and Sputnik-V have >80 % effectivness. It lowers chances of infection and death.
https://www.clinicalmicrobiologyandinfection.com/article/S1198-743X(21)00639-X/fulltext
You mostly cherrypick evidence. For example Gibraltar does not really have stable population. Many people cross borders and move because it is so small and isolated.
Also this "fat people problem" is getting kinda anoying. Yes, they are generally more likely to die. But the point is that unvaccinated fat people die much more than vaccinated fat people.